| Posted by Sonia Richards on 23/05/2020 | 0 Comments |
Those of you who have trained in IEMT, particularly if you attended one of my trainings, will know how much emphasis we put on really listening to language. Our own and that of others. This week on Facebook, Andrew Austin posted an old article that he wrote some years ago on the subject of language in medicine and the Post Hypnotic Suggestions that many medics use, either purposely or inadvertently. This got me thinking about my own experience within the medical profession and as a service user, with particular emphasis on the work that I do with pregnant women and their partners.
When women become pregnant a whole new dynamic seems to occur for them. They seem to stop being merely a woman who happens to be pregnant, which is after all a normal physiological event, but to somehow be viewed as though they have an illness, and as a result are often treated like patients. Also there is a conferred status shift between the woman and her caregivers which can be overt or more often quite subtle. Some caregivers even start to speak to women in a patronising way as if they have suddenly become a child again or somehow less intelligent.
Certain caregivers confer some sort of ownership onto pregnant women and when referring to them will use terms such as, “my lady…” or “my group of ladies…”. Women attending clinics or a unit for birth, often have their name/identity dismissed and become the “Primip” (first pregnancy mum) in room 3 or the “Multip” (mum with more that one pregnancy before) in room 1, “The Section in room 5” (Caesarian Section) and so on. This depersonalisation is one of the many reasons why some women’s experience of birthing especially in hospitals, can be less than a positive experience. Home birth women often have a much more positive experience and in some cases the attending midwife will be a person who has been seeing them throughout their pregnancy and as such they have built up a special relationship, a bond if you will. However in some cases, more usually in a hospital setting, their name and age may be dismissed and they will be called a “Good girl”, or as has become the fashion lately , “That’s it lovely, go on hun…”. I feel sometimes like they will be patted on the head like a dog!
The above language changes all seem very mild and may not be of concern to some women, or they may just choose to ignore it in the great scheme of things. However for some, it will rankle, and such niggling feelings during birthing can expand exponentially and may begin to create changes in hormonal status that is not conducive for birthing, i.e. a drop in oxytocin and a rise in cortisol and adrenalin levels.
Some of the language of pregnancy and birthing however is not so mild and benign, such as being called a “Good girl”. It can be highly fear inducing and I have seen and heard only too often of the trauma that can result in how women are spoken to. Not only the words spoken, but the tone, delivery and body language.
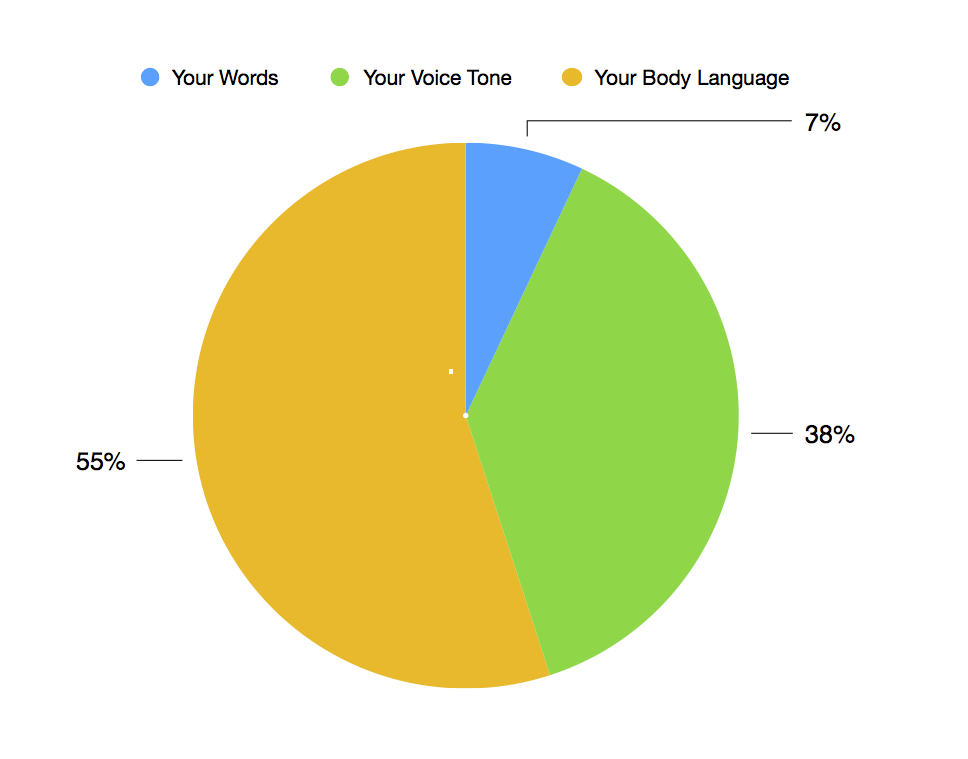
The Albert Mehrabian model is often used to demonstrate this when looking at communication within organisations and relationships. According to the renowned Psychologist, the above three elements account for our perception of another person. The percentages may not be exact, however for most people they will be very close to the mark.
The following is a true event. It may sound extreme, however, such language is still being used with clients that I work with and relative physiological and psychological morbidity can occur:
A former Hypnobirthing client of mine, was told she had tested borderline for Gestational Diabetes. There are different levels of Gestational Diabetes that occur in a small percentage of pregnancy and there are different modes of treatment and management required. In this case it was borderline and could most likely have been managed via dietary changes. She was 36 weeks pregnant and planning a home birth. On discussing her options with the doctor and clearly stating that she was not ready to consider induction or Caesarian Section as was being suggested, the doctor told her in no uncertain terms that she was putting her baby in danger and could kill her baby if she didn’t agree to be induced at 38 weeks. The baby was not measuring large, there were no indications of heart issues and she was a slim healthy lady herself.
This lady was so traumatised by what she has been told, that she called me just after the appointment and that very evening went into early labour, possibly due to the shock. She birthed her baby wonderfully at the hospital using Hypnobirthing techniques. The baby was born healthy, weighing just over 5.6lbs (2.5 Kg) and did not need to be incubated.
A few months after the baby was born, the client contacted me, as she was experiencing emotional trauma. IEMT, in particular the PTSD model and some episodic memory work, proved invaluable for this lady. She was finding it impossible to let go of what she had been told by the doctor. It was not the unexpected labour or the birth that proved to be her Lynch Pin, it was the memory of what was said to her, and how it was said, that she was finding so difficult to let go of and as a result this was detracting from her experience of motherhood. The release for this lady was wonderful. She found a new joy in being a mum and I was very honoured to be invited to the baby’s Christening a few months later.
One way that I work with birth trauma is to listen to the story of their experience if they wish to speak about it. Some won’t want to of course. Often, birth trauma is not a result of the actual labour or birthing experience, but what was or wasn’t said or done, both by the caregivers and the clients. There will be a lot of “If only I had said this… or done that”. Clients may feel like they weren’t listened to or that their wishes were ignored or even dismissed, hence if a woman wants to tell her story I am always happy to listen. For some women the Lynch Pin is the memory of a ‘certain look’ from a caregiver that can seem dismissive, derogatory or even hostile that seers into their brains at such a highly emotional time in their life.
As a result of the above incident, I arranged via the Chair of the Maternity Services Liaison Committee, of which I was a member, to meet with the Consultant in charge of staff training at the hospital concerned. A plan was formulated to study the use of language by medical staff during maternity care. Disappointingly during that meeting, when talking about how he would have handled the case, the Consultant stated, “I would have allowed her to get to 40 weeks before talking about induction.” My college and I reacted strongly to this statement. The term “allowed” is often used in maternity care, and most care givers do not see this as an issue. It is the woman who’s permission must be given, as all decisions are hers to make as part of her ‘informed choice’ and ‘birth rights’. These are all too often ignored or dismissed by medical staff. The Consultant realised his error at once and to his credit apologised and subsequently gave his backing for the study. Sadly this study never saw the light of day due to the appointment of a new Trust Chief Executive and the funding being stopped.
In IEMT we carefully monitor clients use of language both verbal and written, as so much information is there to be gleaned. Emails, phone calls the pre-session questionnaires / intake forms are all sources of invaluable information. Patterns of Chronicity and many identity discrepancies and mismatches can be discerned and are a great way to prepare for up coming sessions.
As an IEMT Practitioner ‘you’ need to be mindful of “your” language, both in client sessions and everyday life. Take care that ‘you’ do not paraphrase language used by ‘your’ clients, thus putting ‘your’ own interpretation onto their experience. Are ‘you’, a probably, maybe, sort of person? Do ‘you’ tend to “What if” or “If only?” How integrated are the aspects of ‘your’ own identity? All of this will seep into ‘your’ own language as those who have trained with me are well, aware and yes even ‘I’ on occasion say “You” instead of “I”, but that’s all for another blog…
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|